Healthcare has spent the past decade chasing scale. More patient records. More connected systems. More dashboards. More AI. The assumption has been simple: if we collect enough data, better decisions will follow.
But what if the opposite is becoming true?
Today, the limiting factor isn’t access to data. It’s confidence in the data we already have. Without trust, every new dataset adds another layer of uncertainty. More information can increase cognitive load, dilute the signal with noise, and make both clinicians and AI less reliable.
The competitive advantage in digital health is no longer more data. It’s trusted data.
The myth of “more is better”
Many healthcare organisations still measure digital maturity by connection counts, data volume or platform scale. Those metrics matter, but they don’t tell you whether better decisions are being made.
Recent research highlights three assumptions that healthcare data leaders should challenge:
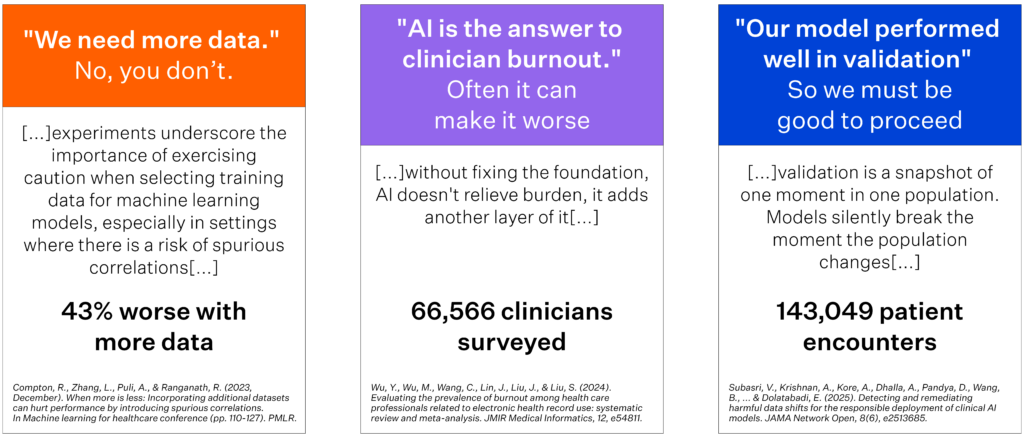
Source: Compton et al. (2023); Wu et al. (2024); Subasri et al. (2025).
The evidence is sobering:
- Adding more datasets can reduce machine learning performance by introducing spurious correlations.
- AI doesn’t automatically reduce clinician burnout. When built on poor workflows or unreliable information, it often adds another layer of administrative burden.
- Strong validation results are only a snapshot in time. Clinical AI can silently degrade as populations, workflows or laboratory practices change.
The lesson is clear: quality matters more than quantity.
Trusted data is a clinical capability.
Healthcare data only creates value when someone can act on it with confidence.
That could be a clinician deciding on treatment, an executive allocating resources, a commissioner redesigning services, or a researcher evaluating outcomes. In every case, the question isn’t Does the data exist?, It’s Can we trust it enough to make the right decision?
Unfortunately, trust remains one of healthcare’s biggest blind spots.
Electronic health records contain enormous clinical value, yet data quality varies due to inconsistent coding, incomplete documentation, workflow differences, delayed updates, and human behaviour. Information may be technically correct but clinically misleading. A record may exist, but no longer reflects reality.
When clinicians lose confidence in the data, they respond rationally. They double-check information, create local workarounds, and rely on personal knowledge rather than digital systems. Productivity falls, while organisational confidence in analytics and AI declines with it.
Trust must be designed, not assumed.
Trusted data isn’t created through a one-off cleansing project. It’s an enterprise capability built through governance, standards, workflow design and accountability.
The emerging METRIC framework illustrates just how broad data quality really is.
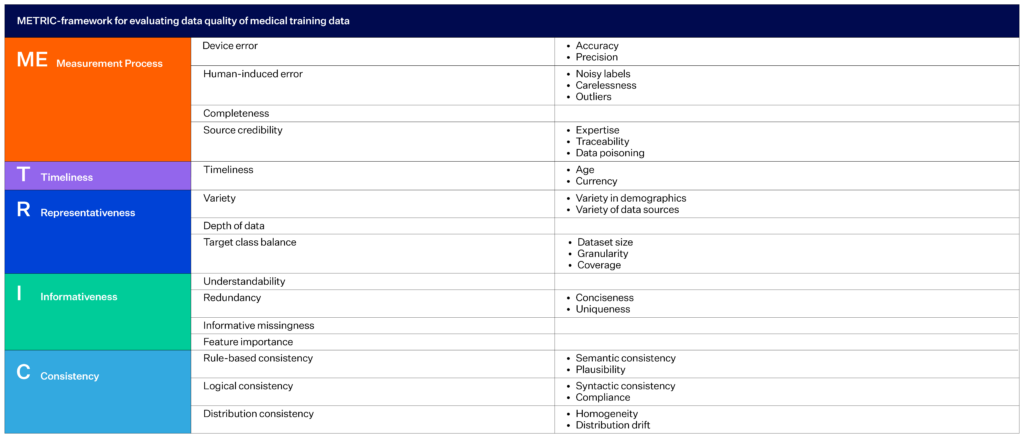
Source: Schwabe et al. (2024).
Rather than measuring quality by completeness alone, the framework evaluates five dimensions:
- Measurement – accuracy, precision and credible data sources
- Timeliness – whether information remains current
- Representativeness – diversity, coverage and dataset balance
- Informativeness – meaningful, unique and understandable information
- Consistency – logical, semantic and distribution consistency
Together, these dimensions determine whether data is trustworthy enough for clinical decision-making and AI.
AI makes trusted data even more important.
AI doesn’t reduce the need for governance. It amplifies it.
A model trained in one hospital can perform very differently when deployed in another. Population characteristics change. Clinical pathways evolve. Laboratory methods differ. Without continuous monitoring, models can drift while appearing to function normally.
This shifts the executive conversation away from “Did the pilot succeed?” towards “Can we continuously trust this model in live clinical practice?”
That’s a far more important question.
The next competitive advantage.
Healthcare organisations often pursue growth through new features, larger platforms or expanding datasets.
But sustainable growth depends on something less visible: trust transfer.
Clinicians adopt systems they trust. Executives invest in insights they trust. Governance teams approve technologies they can defend.
Trust becomes the multiplier that allows every other digital investment to deliver value.
The organisations that succeed over the next decade won’t necessarily collect the most data. They’ll build the confidence to use it.
Because more data creates more possibilities.
Trusted data creates better decisions.
Authored by Tom Varghese, Global Product Marketing & Growth Manager at Orion Health.
References
- Catapan, S. C., Sazon, H., Zheng, S., Gallegos Rejas, V., Mendis, R., Santiago, P. H. R., & Kelly, J. T. (2025). A systematic review of consumers’ and healthcare professionals’ trust in digital healthcare. npj Digital Medicine, 8, 115.
- Ghalavand, H., Shirshahi, S., Rahimi, A., Zarrinabadi, Z., & Amani, F. (2024). Common data quality elements for health information systems: A systematic review. BMC Medical Informatics and Decision Making, 24, 243.
- Mistry, P., Maguire, D., Chikwira, L., & Lindsay, T. (2022). Interoperability is more than technology: The role of culture and leadership in joined up care. The King’s Fund.
- Näher, A. F., Vorisek, C. N., Klopfenstein, S. A. I., Lehne, M., Thun, S., Alsalamah, S., Pujari, S., Heider, D., Ahrens, W., Pigeot, I., Marckmann, G., Jenny, M. A., Renard, B. Y., von Kleist, M., Wieler, L. H., Balzer, F., & Grabenhenrich, L. (2023). Secondary data for global health digitalisation. The Lancet Digital Health, 5(2), e93 to e101.
- NHS England. (2026). Artificial intelligence guidance for information governance professionals. NHS England Digital.
- Penev, Y. P., Buchanan, T. R., Ruppert, M. M., Liu, M., Shekouhi, R., Guan, Z., Balch, J., Ozrazgat Baslanti, T., Shickel, B., Loftus, T. J., & Bihorac, A. (2024). Electronic health record data quality and performance assessments: Scoping review. JMIR Medical Informatics, 12, e58130.
- Schwabe, D., Becker, K., Seyferth, M., Klaß, A., & Schäffter, T. (2024). The METRIC framework for assessing data quality for trustworthy AI in medicine: A systematic review. npj Digital Medicine.
- Subasri, V., Krishnan, A., Kore, A., Dhalla, A., Pandya, D., Wang, B., Malkin, D., Razak, F., Verma, A. A., Goldenberg, A., & Dolatabadi, E. (2025). Detecting and remediating harmful data shifts for the responsible deployment of clinical AI models. JAMA Network Open, 8(6), e2513685.
- World Health Organization Regional Office for Europe. (2025). Artificial intelligence is reshaping health systems: State of readiness across the WHO European Region. World Health Organization.


